
URINARY TRACT INFECTION (UTI)
5 Key Points:
- UTI is more common in women, especially those who are sexually active and post-menopause
- Underlying treatable causes are to be excluded, esp. prostate obstruction, stones, anatomic abnormalies
- With increasing antibiotic-resistance, a urine culture is essential in determining the type of bacteria and appropriate antibiotic
- It is important to treat bladder infections (cystitis) early before the bacteria disseminate to the kidney to cause pyelonephritis
- A 5-day course of antibiotics is adequate in uncomplicated UTI, but more complicated UTIs require further investigations and a longer course
When bacteria gets into the bladder, it causes an infection (cystitis). Left untreated, the infection goes up to the kidneys to cause a more severe infection (pyelonephritis). Urine infection affects all age groups but sexually active and post-menopausal women are especially prone to UTI. The symptoms include frequency of urination, lower abdominal pain, burning sensation in the urine passage, cloudy, smelly urine and frank blood in the urine. When the infection affects the kidneys, loin pain, fever, chills and even septic shock can occur.
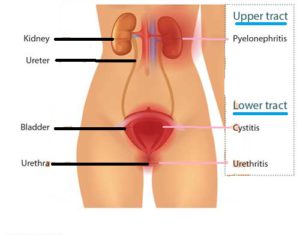
UTI is also more likely to occur when there is a congenital abnormality in the urinary tract [Fig 1], e.g. ureterocoele, duplex kidney [1a], vesico-ureteral reflux [1b]. Diabetic patients are also more likely to get UTI due to the excess sugar in their urine. The other predisposing causes are stagnant urine in the bladder from obstruction from BPH or weak bladder (hypotonic bladder).
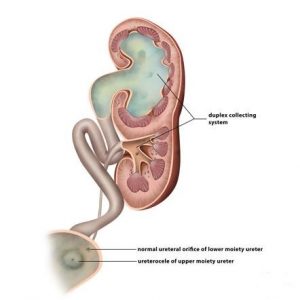
Fig 1a. Duplex kidney with ureterocoele
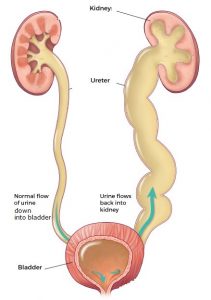
Fig 1b. VU reflux
Diagnosis
1. Urine dipstick [Fig 2]. The finding of red and white blood cells in the urine is typical of UTI. A quick dipstick test is the combur 10 which takes only 1 minute to do. A positive reaction to white blood cells and nitrites confirms the presence of bacteria.

Fig 2. Urine dipstick is a quick initial test for UTI
2. Urine culture [Fig 3]. Confirmation of UTI is best done from a mid-stream urine specimen. As there are many types of bacteria, a culture should always be done to isolate the offending bacteria and identify the most appropriate antibiotic. Most laboratories can give the result in 48 hours.

Fig 3.Urine culture to confirm type of bacteria and the appropriate antibiotic
3. Ultrasound. A screening ultrasound can easily be done in the clinic. This may reveal bladder or kidney stones as the underlying source [Fig 4].

Fig 4. Ultrasound of the bladder showing a stone causing recurrent UTI
4. Xrays [Fig 5]. If ultrasound reveals a stone or an abnormal-looking kidney, contrast X-ray studies of the urinary tract (IVU) is indicated [5a]. They are also recommended in recurrent UTI to exclude an abnormal urinary system e.g. duplex ureter in which urine can reflux up into the kidney and ultimately, cause kidney damage. A CT urography scan can also be done with the advantage that a 3-dimensional image can be constructed [5b].

5a. IVU of an infected left kidney from stones
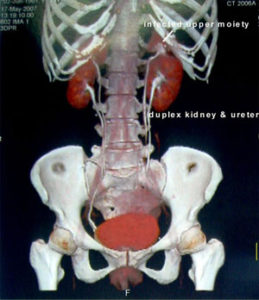
5b. CT scan showing duplex left kidney
5. Cystoscopy [Fig 6]. Endoscopic inspection of the bladder can also rule out anatomic bladder disease, eg. diverticulum, enlarged prostate. The scope can easily be done under local anaesthesia.
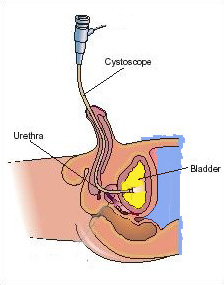

Fig 6. Flexible cystoscope to visualize the bladder and prostate
Treatment
The mainstay of UTI treatment is appropriate and adequate antibiotic course. Uncomplicated UTI require only 5 days of antibiotics. Complicated require at least 10 to 14 days, e.g. in infections of the prostate, kidney, diabetes. It is important to obtain a urine culture as the result will help the doctor select the most effective drug. With widespread use of antibiotics, antibiotic resistance is very prevalent.
The most common drugs for uncomplicated UTIs are trimethoprim/sulfamethoxazole (Bactrim), Augmentin and ciprofloxacin (Ciprobay). It is important to complete the full course of treatment because symptoms usually disappear before the infection is fully cleared. Pregnant woman who develop a UTI should be treated promptly, bearing in mind that only certain antibiotics are safe for the foetus.
Drugs can be given to relieve the pain of urination, e.g. flavoxates (Genurin, Urispas). Urine alkalinizing agents such as citrate (Urocit K, Citravescent) can also alleviate the irritative symptoms and may help prevent UTI too. Probiotics and cranberry juice have not been proven to prevent UTI.
UTI In Females
Women are more prone to urine infection because their urethra is much shorter and the opening is sited just next to the vagina. Typically, young girls get their first cystitis when they become sexually active. Post-menopausal women are also prone to urine infection because the dry vagina and urethra is less resistant to bacteria. The types of bacteria that get into the bladder originate from the faeces. Hence, maintaining local hygiene is important in preventing UTI. When the infection proves difficult to treat or is recurrent, an underlying cause should always be suspected, e.g. stones, duplex system, refluxing ureter. The UTI may also be related to fungal infection in the vagina.
Diagnosis
Examination of the vulva may reveal an inflamed opening (caruncle) or vagina inflammation (vaginitis).
Recurrent UTIs
Many women suffer from frequent UTIs. Nearly 20% of women who have a UTI will have another. It is well known that some women are just more prone to recurrent attacks. Women who are particularly prone are those whose urethra opening is close to the vagina; allowing bacteria to enter the urethra more easily during sex. Another common reason for recurrent UTI is the persistence of bacteria that was not eradicated the last time round. The widespread use of antibiotics have resulted in resistant strains which remain in the lining of the vagina and urethra. Doctors often give antibiotics based on “best guess” but do not realize that if the bacteria is only partially sensitive to the antibiotics, the bacteria will continue to thrive. Hence, it is important to do a urine culture prior to starting antibiotics to identify these resistant strains of bacteria.
Women with frequent UTI and no identifiable cause will benefit from preventive antibiotic therapy. About 4 out of 5 women who have a UTI get another within 18 months. A woman who has frequent recurrences (3 or more a year) are candidates for prophylactic antibiotics:
• Low dose antibiotic taken at night for 3 months, e.g. bactrim, nitrofurantoin
• Single dose antibiotic immediately after sexual intercourse
Additional steps that a woman can take to avoid an infection are:
• Drinking plenty of water every day (2 litres). Drinking cranberry juice may help but the scientific evidence is weak.
• Not holding the bladder for too long because stale urine is a good medium for bacteria
• Emptying their bladder immediately after sexual intercourse
UTI In Males
UTI is unusual in men. A common and often missed underlying cause is foreskin infection (balanitis). Young men (20 to 50 years) are also prone to prostate infection (prostatitis). [Fig 7]. Many of them are assumed to have simple UTI and given a short course of antibiotics, which is not sufficient in eradicating the bacteria that are actually residing inside the prostate, resulting in a re-infection after the antibiotic is finished.
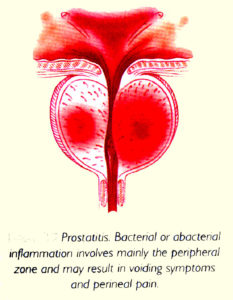
Fig 7. Prostatitis is a common cause of UTI in younger men
In older men (above 50 years), it usually stems from stagnant urine in the bladder caused by an enlarged prostate (BPH) [Fig 8].
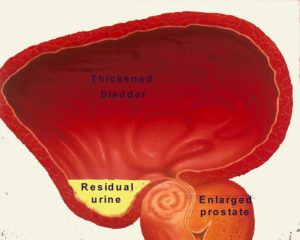
Fig 8. BPH in older men causing retention of urine
Diagnosis
UTI in men require a proper physical examination to reveal underlying causes, e.g. a tight foreskin (phimosis) which traps dirt beneath and promotes bacterial overgrowth to infect the foreskin over the head of the penis (balanitis) [Fig 9].
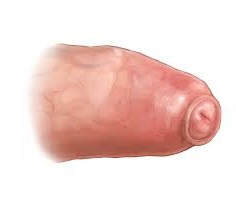
Fig 9a. Phimosis

Fig 9b. Balanitis from phimosis
Prostatitis itself is a clinical diagnosis. A physical exam is done to check for pelvic / groin tenderness and a digital rectal exam will reveal a swollen (boggy) and tender prostate [Fig 10].
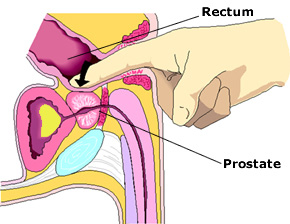
Fig 10. Prostate examination to detect prostatitis
If sexually transmitted disease is suspected, penile swab and blood tests can be done.
Types
Prostatitis fall into the following categories:
q) acute bacterial prostatitis
b) chronic bacterial prostatitis
c) nonbacterial prostatitis, prostatodynia and chronic pelvic pain syndrome
a) Acute bacterial prostatitis
The symptoms come on suddenly and may include:
• Fever and chills
• Pain in the pelvis, lower back or groin
• Burning pain during urination (dysuria)
• Frequent urination
• Bloody urine
• Difficulty emptying the bladder and even sudden painful retention of urine
Acute prostatitis can be a serious condition and requires intravenous antibiotics until the fever subsides, followed by oral antibiotics for at least 3 weeks.
b) Chronic bacterial prostatitis
Chronic bacterial prostatitis develops more slowly and usually not associated with high fever. The symptoms of pain tend to wax and wane and include:
• Frequent and urgent need to urinate, both day and night
• Dull ache in the pelvic area, lower back and scrotum
• Pain referred to the penis tip at the end of micturition
• Hesitancy when initiating a urine stream
• Blood in urine or semen
• Pain after ejaculation
c) Chronic non-bacterial prostatitis
Chronic non-bacterial prostatitis is due to persistent non-infective inflammation of the prostate. The symptoms are similar to those of chronic bacterial prostatitis. A man is assumed to have non-bacterial prostatitis only after an adequate course of antibiotics has been given. The only way to prove whether the prostatitis is bacterial or not is from direct culture of the prostate / seminal fluid. Nonbacterial prostatitis may also be chemical in nature, e.g. from reflux of urine into the prostate as a result of non-relaxing urinary sphincter e.g. psychological stress, excess caffeine.
Summary
UTI is a very common occurrence especially in women. In men, prostate infection (prostatitis) is the more likely cause and this can be chronic. It is important to get a urine culture as antibiotic resistance is very common and “best-guess” antibiotic may not work. Underlying anatomic causes and stones need to be excluded if the UTI is recurrent. Women prone to recurrent UTI will benefit from prophylactic antibiotics.